Product Detail
VAULT Bronze
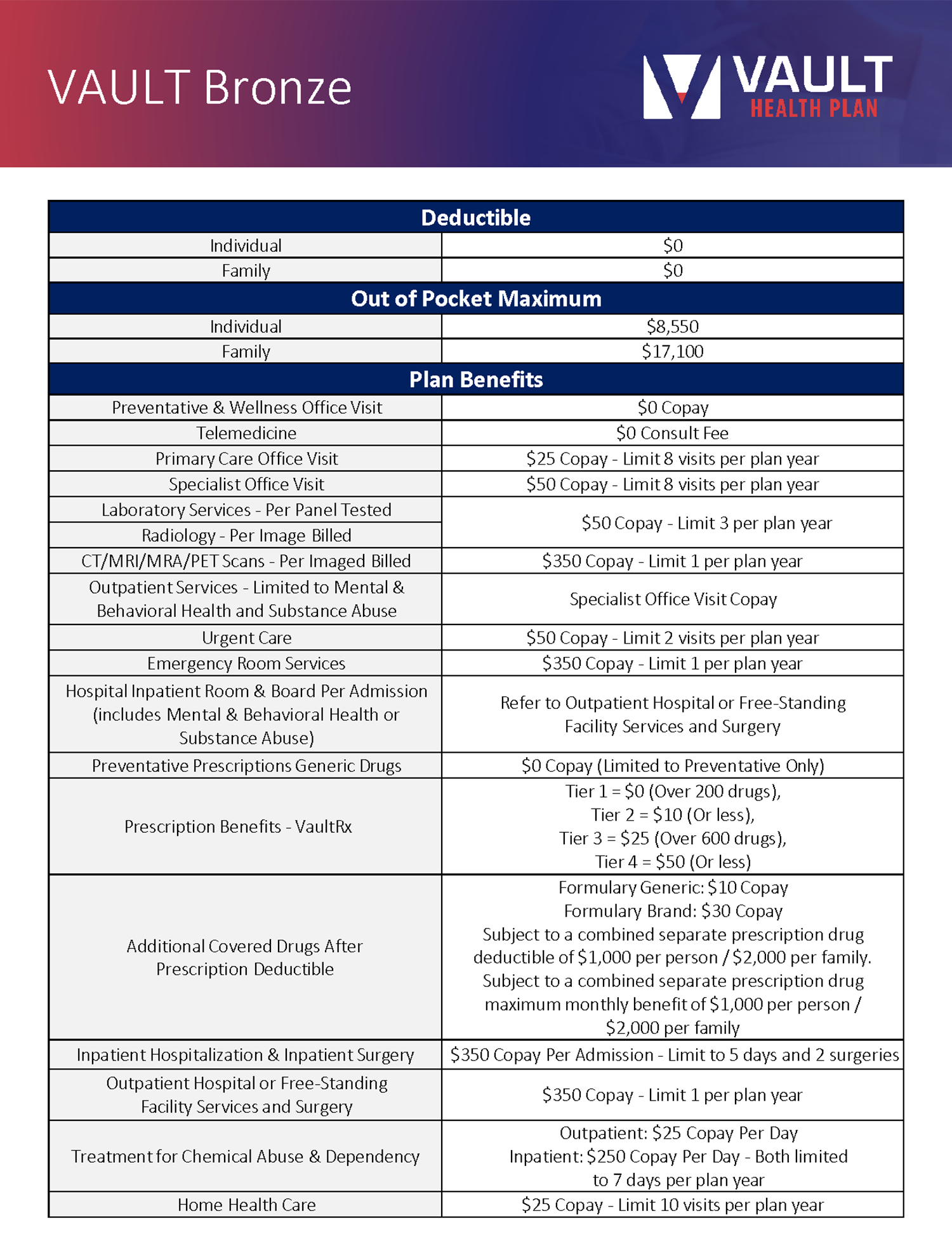
Vault Bronze
- Preventive Services
- Co-Pay Visits for PCP/SPC/UC/ER
- Labs/Imaging, Hospitalization and Surgery, Preferred Formulary Prescription Coverage, Unlimited $0 Telehealth Consults
- Access to a dedicated clinical navigator –find highly rated doctors, review medical bills and resolve disputes, access quality ratings and more
Click here for Vault Bronze Brochure
Please Note: Please refer to the Schedule of Benefits and Description of Coverage for the official list of Benefits Coverage, Limitations, and Exclusions. If plan comparison above differs from the Schedule of Benefits and Description of Coverage, the Schedule of Benefits and Description of Coverage will govern.
Important Note Regarding Preventive or Diagnostic Services Performed at a Hospital: Services performed at a hospital not related to inpatient hospitalization or surgery will not be covered. Any tests or imaging sent to a hospital by a physician or outpatient facility to be read or reviewed will not be covered. Member will be liable for 100% of the cost when this occurs. It is the members responsibility to first check with their provider to verify these services are not being sent to a hospital. This can be an issue for preventative mammograms, Member is advised to clarify with provider ahead of time.
Important Note Regarding IP/OP/Surgery Services Performed at a Hospital:
This plan does not utilize a network for any facilities. All services performed in a medical facility (for example, a hospital as opposed to a primary care physician’s office) will be subject to Reference Based Pricing (RBP) reimbursements based on a multiple of the Medicare Reimbursement Rate. Prior authorization needs to be obtained for some benefits offered in the plan. Please refer to the schedule of benefits for a more in-depth list of Benefit Coverage, Limitations and Exclusions. Out of Network services, and services provided at a hospital, will not be covered, unless otherwise specified.
Summary of Benefits and Description of Coverage
Summary of Benefits w/ Exclusions
